
By Amy Fiske, PhD (Associate Professor of Clinical Psychology, West Virginia University)
Missing the Group Most at Risk
This is National Suicide Prevention Week. Much will be said and written this week about suicide and how to prevent it. Most of it will not even mention the group at greatest risk of suicide: older men.
Suicide rates in men over age 70 are higher than in any other demographic group worldwide, according to a recent report by the World Health Organization. In the United States, the rate of suicide for men 70 and older is more than double the overall suicide rate [calculated from information available here: http://www.cdc.gov/injury/wisqars/]
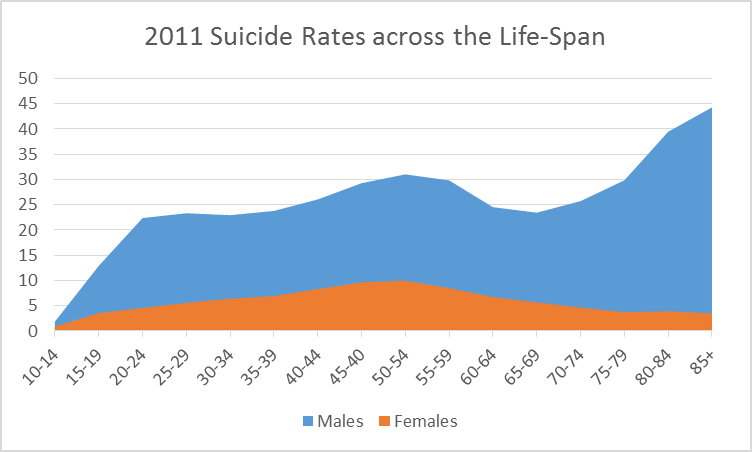
Note: rates are per 100,000 population from CDC WISQARS system.
The tragic recent death of Robin Williams at age 63 has brought attention to the dramatically increasing rates of suicide among the middle aged (45-64 years age group). This increase in suicide rates among the middle aged is another reason to pay attention to the problem of suicide in older men (who have even higher rates). Researchers have long been predicting that the number of older adult suicides will increase along with the dramatic expansion of this age group due to the aging of Baby Boomers like Robin Williams.
Where’s the Response?
Even though it is well-established that older men are at the highest risk of suicide, you would not know that by looking at our official suicide prevention efforts.
Most of the funding for suicide prevention programs in the U.S. is targeted to youth suicide prevention. There is a great need for suicide prevention in this age group, and this funding is laudable. But we also need funding for suicide prevention in older adults.
Recently, the Substance Abuse and Mental Health Services Administration (SAMHSA) released a draft of its strategic plan for 2015-2018. One of the goals focused on prevention of suicide in high risk populations. Older men were not even mentioned.
Even the World Health Organization (WHO) report released last week downplayed the risk of suicide in older adults. “Suicide occurs all over the world and can take place at almost any age. Globally, suicide rates are highest in people aged 70 years and over. In some countries, however, the highest rates are found among the young. Notably, suicide is the second leading cause of death in 15-29 year-olds globally.”
Is Late Life Suicide Understandable?
Most people think suicide is an understandable reaction to the misery of growing older and particularly to the physical health problems that accompany aging. There are two problems with that logic:
- Late life is not miserable for most people. Older adults are less likely than their younger counterparts to suffer from anxiety disorders, depression, and many other psychiatric disorders, and they display more positivity and report higher levels of well-being.
- Although it is true that physical health generally declines with age, the vast majority of older adults do not become suicidal when their health declines. Physical health problems are often part of the picture when an older man dies by suicide, but the types of illnesses might not be what you think. They are not all terminal or painful conditions. They include incontinence, poor vision and hearing problems. Cancer is a risk factor for suicide in late life, but research suggests that much of the risk is seen at the onset of the disease. This raises questions about adaptation to the diagnosis.
Is that what happened to Robin Williams? According to news reports, his wife indicated that he had Parkinson’s disease, and that he had not yet come to terms with the idea of telling people about it. Could his suicide be related to difficulty adapting to the disease?
So Why Do Some Older Men Die By Suicide?
The most prominent risk factor for suicide in late life, as at other ages, is depression. Alcohol use disorders are also implicated. Depression is often undetected and untreated in older adults. Fortunately, some approaches to improving treatment of depression in older adults are effective. Medications and psychotherapy significantly reduce depressive symptoms. Interestingly, when given thorough descriptions of these treatments, older adults state a preference for receiving psychologically based treatments rather than medication.
The Bottom Line
Suicide in older men is an important public health problem that can be prevented, but nobody seems to be noticing. We need to wake up and do something about it. National Suicide Prevention Week would be a great time to step up.
Here’s What You Can Do
- Understand and explain to others that depression and suicide are not a normal part of aging.
- Know the warning signs for suicide and notice if older adults in your life are at risk. Take action if they are. Call the National Suicide Prevention Lifeline: 800-273-8255 or Friendship Line for the Elderly: 800-971-0016, an accredited national hotline/warmline that focuses specifically on older adults.
- Learn Read APA’s Depression and Suicide in Older Adults Resource Guide and the National Institute on Aging’s Age Page on Depression.
Biography
Dr. Fiske received her Bachelor of Arts degree in English from Stanford University, her Master of Arts degree in social psychology from San Francisco State University, and her Doctor of Philosophy degree in clinical psychology with a focus on aging from the University of Southern California. She completed an internship at the Veterans Affairs Palo Alto Health Care System. She completed postdoctoral work and a visiting faculty appointment at the University of Southern California and joined the faculty in the Department of Psychology at West Virginia University in 2005. Dr. Fiske was promoted to Associate Professor in 2011 and currently serves the department as Director of Clinical Training and the Coordinator of the Clinical Psychology Program Area. Dr. Fiske’s primary research interests involve the etiology of depression and suicidal behavior in late life and the implications for prevention. She also has interests in the assessment of sleeping problems and treatments for insomnia and other sleep disorders. – See more at: http://psychology.wvu.edu/faculty-staff/faculty-directory/amy-fiske#sthash.dcTvAEhv.dpuf
Image source: iStockPhoto


Good lord I never even thought about older men committing suicide. Thank you for writing this. Very eye opening post. Founder, http://www.counselinginsite.com
LikeLike
Reblogged this on Counseling Insite.
LikeLike
I realize that although the suicide of someones father, brother, husband, or friend can be a tramatic occurance, we need to remember that it was that man’s decision at that moment, and we cannot know his mind at the time. Please respect his wishes.
LikeLike